When musculoskeletal imaging starts backing up, the impact moves quickly beyond radiology. A delayed MRI can hold up orthopedic treatment plans, slow emergency department decisions, frustrate patients waiting for answers, and create more follow-up calls for already busy clinicians. For hospital and imaging leaders, the real issue is broader than scheduling alone. Imaging demand keeps rising, and Vizient has pointed to continued growth in advanced imaging over the coming decade, which puts even more pressure on departments already trying to protect workflow, access, and turnaround.
ED throughput can feel the impact quickly
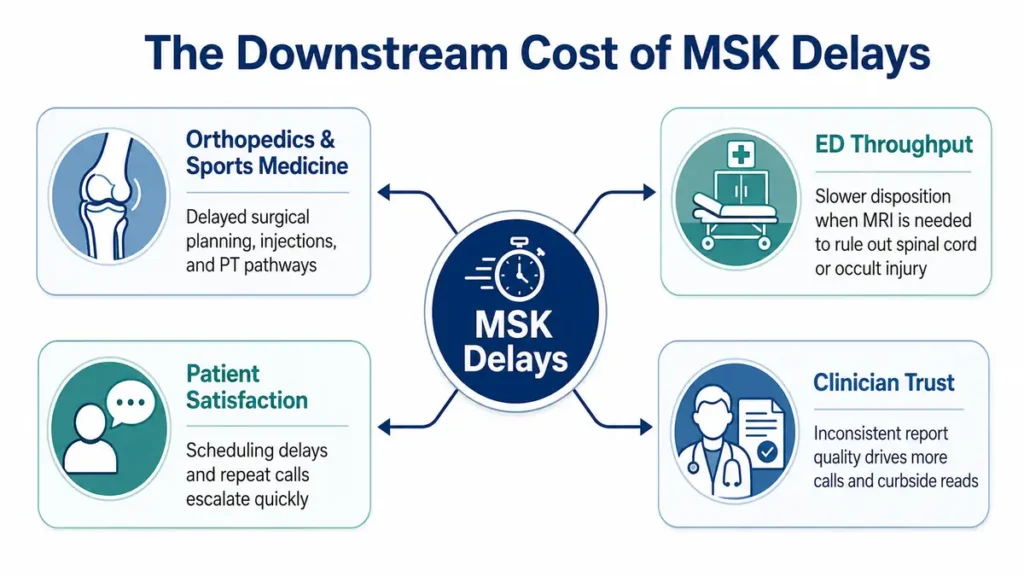
For emergency departments, MRI delays can create a different kind of strain. When a patient needs advanced imaging to clarify a spine issue, occult injury, or another musculoskeletal concern, disposition decisions may slow down while teams wait for imaging access and interpretation. That affects bed availability, staff coordination, and overall throughput. Recent reporting from Becker’s has continued to highlight how radiology staffing pressure and rising imaging demand are shaping access and operational stability in 2026.
The staffing picture adds more pressure to the workflow
This challenge becomes harder when radiology departments are already operating with workforce constraints. The American College of Radiology’s 2026 workforce update pointed to continued attrition pressures, including higher attrition in practices with rural sites and meaningful variation across practice settings. That kind of strain can make it more difficult to maintain steady turnaround, especially in service lines where advanced imaging and subspecialty reads carry heavier clinical weight.
Delays also change the patient experience
Patients may never use the phrase “MRI backlog,” but they feel its effects almost immediately. Delayed scheduling, postponed follow-up conversations, and repeat calls to check status all shape the patient experience. When an injured patient is waiting to learn whether surgery, physical therapy, or another intervention is next, even a short delay can create frustration. Imaging leaders usually see this first through call volume, scheduling pressure, and front-desk strain rather than through formal complaints.
Clinician trust can erode when reports feel inconsistent
There is also a less visible downstream cost: extra physician time. When clinicians feel uncertain about report consistency, they tend to make more follow-up calls, ask for informal curbside reads, or seek additional clarification before moving ahead with care plans. That added friction may not show up in a standard turnaround-time report, yet it has a real operational cost. In busy orthopedic, ED, and multispecialty settings, consistent interpretation quality matters just as much as speed.
Why this issue keeps getting more attention
The broader imaging environment helps explain why this topic is gaining traction. Demand for advanced imaging continues to climb, and hospitals are under steady pressure to support more complex studies while maintaining flow across departments. Recent industry reporting has kept radiology staffing, AI adoption, and operational resilience in focus because leaders are trying to manage growing volumes while protecting workflow quality.
 A practical checklist for imaging leaders
A practical checklist for imaging leaders
- Review where MRI turnaround delays are creating downstream scheduling friction for orthopedics, sports medicine, or spine care.
- Track whether ED disposition delays are tied to MRI access, interpretation timing, or both.
- Look at repeat patient calls, rescheduling patterns, and staff time spent managing delayed follow-up
- Assess whether report consistency is supporting clinician confidence or driving extra clarification calls.
- Identify where workflow support or subspecialty interpretation could reduce friction across departments.
Workflow support matters when MSK demand rises
For hospital imaging leaders, the takeaway goes beyond scanner utilization. MSK delays influence orthopedic schedules, ED decision-making, patient communication, and physician trust in ways that compound over time. Strong radiology support can help protect more than turnaround time. It can help preserve care continuity across departments that rely on imaging to keep treatment moving. That becomes even more important when departments are balancing MRI demand, staffing strain, and the need for clear subspecialty interpretation.
FAQs
Why do MSK imaging delays affect departments outside radiology? Because orthopedic care plans, therapy decisions, injections, and some ED dispositions depend on timely MRI access and interpretation. A delay in imaging often becomes a delay in next-step care.
Why does clinician trust come into the conversation? When report consistency feels uneven, referring physicians often spend more time calling for clarification or seeking additional review. That adds friction across the workflow and can influence how the imaging department is perceived.
Why is this issue getting more attention in 2026? Advanced imaging demand continues to rise while workforce pressure remains a concern, which makes turnaround, prioritization, and operational consistency more important for hospital imaging teams.
How Vesta Can Help
When musculoskeletal imaging delays begin affecting orthopedic planning, emergency department flow, patient communication, and clinician confidence, radiology support needs to do more than keep studies moving. It needs to help protect consistency across the broader care pathway.
Vesta Teleradiology supports hospitals and imaging providers with flexible radiology coverage, subspecialty interpretation, and workflow-minded support designed to help reduce friction where delays tend to spread. With 24/7 service, U.S. board-certified radiologists, and experience supporting facilities across multiple modalities, Vesta helps organizations strengthen turnaround, improve reliability, and support better continuity across the imaging workflow.
Sources
https://www.washingtonpost.com/health/2025/04/05/ai-machine-learning-radiology-software/


 3) Smooth scheduling around your true capacity
3) Smooth scheduling around your true capacity