
Growth in imaging services usually looks positive on paper. More referrals, broader service lines, and greater modality depth can all signal momentum. The operational picture gets more complicated once that growth starts stretching reading coverage, scheduling coordination, and subspecialty access. For radiology directors, that is often the point where planning needs to shift from volume management to infrastructure strategy. As hospitals and imaging centers expand into more advanced imaging, the effects reach far beyond scanner utilization. CT, MRI, mammography, nuclear medicine, and PET each bring their own workflow patterns, staffing implications, and interpretation needs.
Coverage models can drift out of sync with the modality mix
This is where radiology directors often run into a hidden problem. The original coverage structure may have worked well for a simpler imaging environment, then slowly becomes less aligned with the department’s current reality. Turnaround pressure rises in certain modalities. Overnight support feels harder to balance. Reading assignments become more fragmented. Referring clinicians start asking for more subspecialty input. That usually means the coverage model was built for an earlier stage of growth.
Staffing pressure makes the gap more obvious
Recent workforce data has made that planning challenge even more urgent. The ACR’s 2026 workforce update pointed to continuing attrition pressures across radiology, while Neiman Health Policy Institute has also highlighted higher attrition among several radiologist subgroups and practice settings. For radiology directors, that reinforces a practical point: growth planning and coverage planning can no longer sit in separate conversations.
Subspecialty access becomes a bigger leadership issue
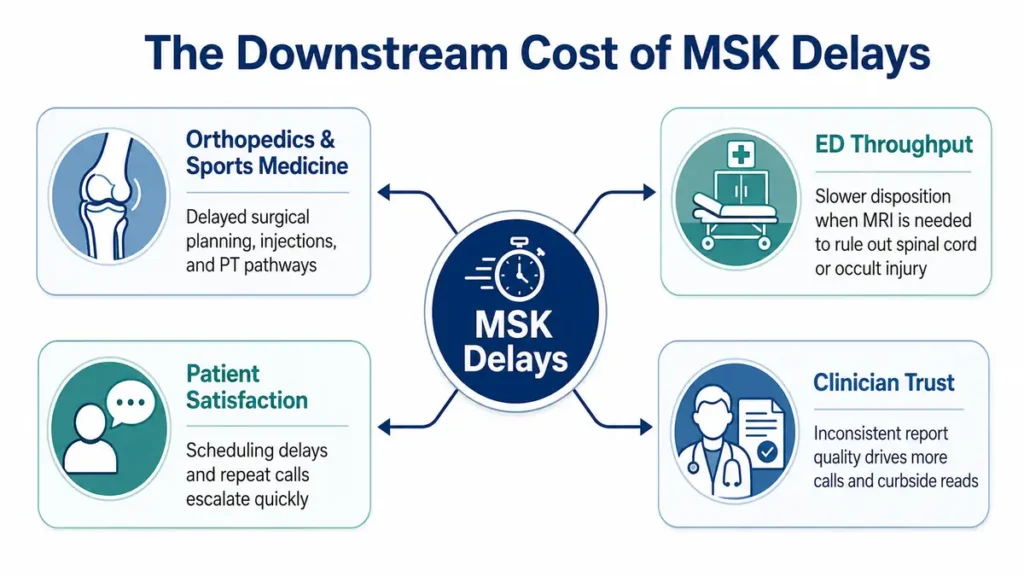
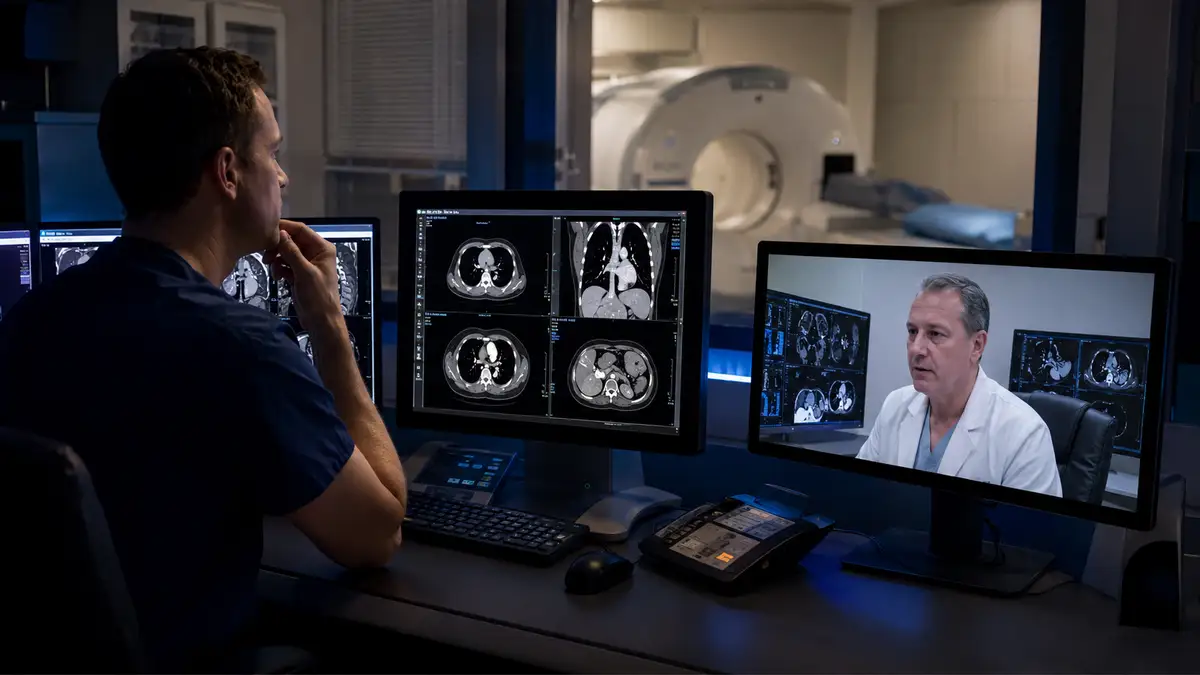
As modality mix broadens, subspecialty interpretation often becomes more important to both clinical quality and referrer confidence. That is especially true in departments where advanced neuro, MSK, breast imaging, or other specialized studies are becoming a larger part of the case mix. A department can continue moving studies through the system, yet still create downstream tension if clinical teams feel they are working without enough interpretive depth in key areas.
Workflow tools matter, but the fit matters more
Technology often enters the conversation at this stage too. The FDA’s public list of AI-enabled medical devices continues to grow, and radiology remains one of the leading categories in that landscape. At the same time, recent national reporting has underscored that AI’s value in radiology depends heavily on how it fits into real-world workflow rather than on novelty alone. Tools that help prioritize time-sensitive studies or streamline repetitive tasks can support busy departments. Tools that add friction tend to create more resistance than relief.
Recent leadership conversations point in the same direction
This broader operational shift has stayed visible in 2026 reporting. Becker’s has continued covering the radiology workforce and the way staffing strain intersects with AI adoption and access. Meanwhile, AHRA’s annual meeting this July will again bring imaging managers and department leaders together around the practical challenges of running imaging operations in a period of continued change.
A planning checklist for radiology directors
- Compare the current coverage model against the department’s actual modality mix, including CT, MRI, breast imaging, nuclear medicine, and PET where applicable.
- Identify where turnaround pressure is clustering by modality, time of day, or service line.
- Review whether overnight, overflow, and subspecialty support still match current operational demands.
- Look for early signs of strain such as fragmented reading assignments, growing call burden, or repeated referrer requests for specialized review.
- Evaluate whether workflow tools are reducing friction or adding another layer of complexity for staff and radiologists.
What radiology directors should plan for next
The planning conversation should start with a few grounded questions. Is the current coverage structure built for today’s modality mix? Are certain studies creating repeated bottlenecks? Does overnight or overflow support still fit the department’s service profile? Are referrers asking for more specialized reads than the current model can comfortably support? Those questions matter because modality expansion often creates pressure gradually. The early signs may look like minor workflow friction, growing call burden, or more scheduling complexity. Over time, those patterns can affect turnaround, staff experience, physician confidence, and the department’s ability to keep growing smoothly. The departments that handle this well usually plan ahead of the pain curve. They look closely at coverage structure, workflow fit, and interpretive depth before operational strain starts showing up everywhere else.
FAQs
Why does modality expansion strain coverage? Because broader imaging services often increase complexity in scheduling, reading assignments, subspecialty needs, and turnaround expectations, even when total volume growth feels manageable.
Why should radiology directors care about coverage alignment? A coverage model that fit a narrower service mix may create friction once advanced imaging becomes a larger share of the department’s work.
How does AI fit into this conversation? AI can support prioritization and efficiency when it fits naturally into workflow. Its value depends on practical implementation and continued clinical oversight.
How Vesta Can Help
As imaging departments expand into broader modality mixes, coverage strategy becomes more important to long-term stability. Vesta Teleradiology helps hospitals and imaging centers support growing demands across CT, MRI, mammography, nuclear medicine, X-ray, and ultrasound with flexible on-site and remote coverage models built around real operational needs. From overnight support and overflow coverage to subspecialty reads and radiologist-led workflow support, Vesta helps radiology leaders build a stronger foundation for growth without adding unnecessary disruption to existing processes.
Sources
https://www.beckershospitalreview.com/radiology/
https://www.washingtonpost.com/health/2025/04/05/ai-machine-learning-radiology-software/
https://www.businessinsider.com/radiology-embraces-generative-ai-to-streamline-productivity-2025-6
 A practical checklist for imaging leaders
A practical checklist for imaging leaders




 Vesta has invested in
Vesta has invested in 




 3) Smooth scheduling around your true capacity
3) Smooth scheduling around your true capacity